Darini Rajasingham-Senanayake is an independent researcher affiliated with the International Centre for Ethnic Studies (ICES) in Sri Lanka.
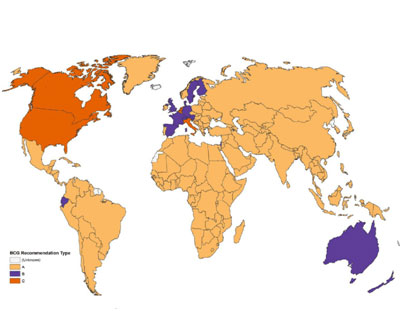
The map from the medical journal Plos Medicine displays BCG vaccination policy by country. Bacillus Calmette-Guérin vaccine is a vaccine primarily used against tuberculosis. Yellow: The country now has a universal BCG vaccination program. Blue: The country used to recommend BCG vaccination for everyone, but now does not. Red: The country never had a universal vaccination program.
COLOMBO, Sri Lanka, Apr 20 2020 (IPS) – Numerous studies in many parts of the world have linked the BCG (Bacillus Calmette-Guerin) vaccination, widely used in the developing world with fewer Coronavirus cases. This is good news for countries that have universal BCG vaccination in tropical Asia and Africa.
Many of these countries cannot afford extended lock downs and curfews since the ensuring economic and supply chain disruption, loss of livelihoods, and poverty could kill more people in the long term.
Originally developed against Tuberculosis (TB), the hundred-year-old BCG vaccine offers broad protection and sharply reduce the incidence of respiratory infections, while also preventing infant deaths from a variety of causes.
According to Prof Luke O’Neill, who has specialised in the study of the vaccine at , a combination of reduced morbidity and mortality could make the 100-year-old BCG vaccination a game-changer in the fight against coronavirus.
While there is no specific cure for Covid-19, the BCG maybe a flak-jacket against the Coronavirus. Experts note that the vaccine seems to “train” the immune system to recognize and respond to a variety of infections, including viruses, bacteria and parasites.
The vaccine is now being tested in several countries including Australia, Germany and Netherlands against the new Coronavirus to protect frontline health workers.
In many countries of the global south’s tropical regions, Covid 19 cases and deaths are in single digits, double digits or hundreds; certainly not in the thousands, unlike in the US and EU, and other temperate regions where the Coronavirus seems more virulent.
This variation has been attributed to differences in climate, cultural norms, mitigation efforts, and health infrastructure. Research indicating that countries whose populations have high levels of BCG vaccination had significantly fewer Covid-19 deaths is highly significant.
Countries that do not have universal policies of BCG vaccination, such as Italy, the Netherlands, and the United States, have been more severely affected compared to countries with universal and long-standing BCG policies, noted Gonzalo Otazu, assistant professor of biomedical sciences at NYIT.
BCG flattens the disease curve since countries that use BCG vaccination programs had a fatality rate of four per million people, while countries without BCG vaccination programs were 10 times more likely to die at a rate of 40 deaths per million people.
While he stressed the research was largely a statistical one and so came with caveats, there was a case for authorities moving to provide a BCG vaccine top-up for everybody age over 70. “This is feasible and should be considered.
BCG in South Asia
In South Asia, the vaccine has been universally used for decades. India and Pakistan started using BCG in 1948 and in Sri Lanka, BCG vaccination became mandatory in 1949, according to the Ministry of Health epidemiology unit. Compared to case numbers in Europe and North America, and relative to population size South Asian countries have registered low numbers and Covid 19 case load.
Three weeks after a pandemic was declared by the World Health Organization (WHO), it is increasingly clear from the Covid 19 data that Asian countries which practice universal BCG vaccination are relatively better positioned to fight Coronavirus despite the crippling curfews that saw millions of migrant labourers walking hundreds of miles and dying in the process to get home.
In addition to BCG, hot and humid tropical weather may be another factor inhibiting the spread and strength of the Covid 19 flu in South Asia. Countries that have a late start of universal BCG policy (Iran, 1984) had high mortality, consistent with the idea that BCG protects the vaccinated elderly population.
Pakistan, a country with 200 million people that did not impose the crippling curfews that neighbouring India and Sri Lanka did, had 4,072 patients with 59 deaths on April 10. Pakistan Prime Minister, Imran Khan, sensibly pointed out that more people would die of poverty caused by lockdowns in the long run.
In Sri Lanka where a brutal curfew was imposed, there have been under 210 Covid 19 cases with 7 deaths, and India a country with more than a billion people has reported 9,000 cases over 3 weeks.
There have been only 12,434 confirmed cases in all 10 Association of Southeast Asian Nations (ASEAN) member states, a miniscule number compared to China, Italy, Spain and the United States, and about the same as Canada, a country of just 37.6 million compared to Southeast Asia’s 622 million.
While lack of testing may be cited as a reason for the relatively low numbers, by now – three weeks after Covid-19 was declared a global pandemic and months after the epidemic in neighbouring China – the region surely should have expected an explosion of cases similar to Italy and Spain.
Clearly in tropical Asian countries, including those with poor health systems the epidemic is far more limited.
This fact raises questions about the Indian and Sri Lankan government’s imposition of economically devastating and socially crippling curfews at the urging of the WHO and Johns Hopkins University (JHU) which is collecting Covid 19 data for a global database, while providing analysis seeming based on simulated pandemic from the mysterious EVENT 201 which was staged last October with the WHO and Gates Foundation and others modeling a fictional novel coronavirus.
WHO’s data and policy recommendations
The bad news is that the World Health Organization (WHO) which is funded by States and big pharmaceutical companies that are rushing to develop Covid 19 vaccines and make big profits,claims on its website that :
“there is no evidence that the Bacille Calmette-Guérin vaccine (BCG) protects people against infection with COVID-19 virus. Two clinical trials addressing this question are underway, and WHO will evaluate the evidence when it is available. In the absence of evidence, WHO does not recommend BCG vaccination for the prevention of COVID-19..
The WHO’s pandemic narrative and call for lockdowns to fight Covid 19 that have caused massive livelihood loss and economic meltdowns in countries like India and Sri Lanka (with the GMOA in tow), have not been modulated by the evidence that the BCG vaccine may act as barrier to the disease.
In short, while the BCG may be a ‘game changer’ in the long run, also in assisting development of herd immunity which would mitigate need for harsh curfews imposed in developing countries that cannot afford shutdowns, the WHO denies this. Heaven forbid that a BCG booster may be the solution in front of us!
There are parallels in the WHO’s denial that the anti-Malaria drug Hydroxychloroquine could be beneficial for Covid 19 patients, while pushing for development of new drugs and vaccines that would bring big profits to drug companies, although researchers in France and China had reported success with the drug.
Increasingly, questions are being raised about the WHO’s Covid19 data, models and analysis. Professor Jay Battacharya of Stanford University has noted that “the claim that coronavirus would kill millions without shelter-in-place orders and quarantines is highly questionable”.
In an interview at the Hoover Institute he observed: “there’s little evidence to confirm that premise—and projections of the death toll could plausibly be orders of magnitude too high.” Fear of Covid-19 is based on its high estimated case fatality rate—2% to 4% of people with confirmed Covid-19, according to the World Health Organization and others.
Drs. Eran Bendavid and Jay Bhattacharya argue that Covid-19 isn’t as deadly as suggested and suggest that the “extraordinary measures” being pushed by the WHO may not be justified. Their argument is that the total number of coronavirus infections is much higher than we think, which mathematically means the mortality rate is much lower.
Exaggeration using war metaphors and nationalism has characterized the WHO’s Covid pandemic narrative. However, the Institute for Health Metrics and Evaluation at the University of Washington School of Medicine now predicts that fewer people will die and fewer hospital beds will be needed compared to estimates from last week.
As of last week, the model predicted the virus will kill 60,000 people in the United States over the next four months 33,000 fewer deaths than estimated last Thursday.
In India, the WHO this week was compelled to correct an exaggeration in a report that claimed that Covid19 had reached level 3 community spread severity. In Sri Lanka several doctors have challenged Covid 19 case numbers and suggested that there is inflation and data manipulation.
We know very little about the virus, but shut down your economies –WHO
“Better to get Corona than see our harvest rotting without customers’, said a famer at the shuttered vegetable wholesale market in Dambulla, central Sri Lanka recently, indicating that there is no trade off to be made between lives and livelihoods as you cannot have one without the other especially in developing countries with high poverty rates.
Farmer suicide rates in South Asia tend to be high due to poverty and debt.
Would the WHO and its director general who called to congratulate the strongman President of Sri Lanka for imposing an indiscriminate and economically destructive month long curfew with military enforcement also count the deaths of farmers, wage-less day labourers and migrant workers who make up the greater part of the labour force who walked hundreds of miles to get home after the imposition of brutal lock downs in India with just 4 hours advanced notice?
WHO’s Covid 19 global media narrative (Al Jazeera CNN, BBC etc), has concentrated on hyping up fear psychosis and groupthink, based on data from Europe and North America, while suppressing mitigating information in the global south.
This has resulted in economically devastating policy making in India and Sri Lanka and a devil’s bargain – an attempt to trade off lives with livelihoods.
The flood of Covid data and information in the media, masks a lack of adequate data disaggregation, comparative analysis and modelling by geographic region and country, as well as, an ahistorical approach. After all, seasonal flu is known to infect over a billion people and kill as many as 750,000 people annually according to the Centers for Disease Control (CDC).
The crippling curfews and destruction of the real economy in India and Sri Lanka reveals serious short comings in national and South Asian (SAARC) regional data analysis, planning and policy making, by the Modi and Rajapaksa governments, and allied medical associations like the Government Medical Officers’ Association (GMOA), as well as, the failure to access regional expertise.
Claims that curfews and lockdowns cannot end until a vaccine is found, reflect bias toward big pharmaceutical companies that also fund research and the WHO, which stand to profit from a new “gold standard” Covonavirrus vaccine.
Surveillance, fear and groupthink
Although the great majority of people who get Corona virus will have mild symptom and survive well, with the creation of a Coronavirus global fear psychosis, economies have been shut down, livelihoods destroyed, and democratic rights compromised as new systems of surveillance and governance are being put in place – for patient network tracking.
In Sri Lanka a brand new USAID funded hospital exclusively for Covid 19 patients has been constructed with promised funding or USD 1.3 million at the former Voice of America compound in Chilaw, equipped with robots, and surveillance technologies “to activate case finding and event-based surveillance, with technical experts for response and preparedness.
The Covid-19 outbreak reveals how pervasive surveillance mechanisms developed in the last decade or so have become. In a strategically located country like Sri Lanka with an under-developed tech sector, foreign countries may access private data platforms via such surveillance platforms is a concern.
Meanwhile, US President Trump’s withdrawal of funds from WHO citing China bias distracts from a more substantive bias at WHO toward big drug companies and related foundations that stand to make a windfall from a Covid 19 vaccine, as well as, related data and policy manipulated that constitute a danger to the health and well-being, lives and livelihood of people everywhere.
This bias is also shared among medical associations like the Government Medical Officers Association (GMOA), in Sri Lanka.
As Professor Nyasa Mboti of Free Town University, wrote: : “by its own admission, WHO seems to have declared Covid19 a pandemic IN ORDER to avert a Covid19 pandemic. This seems illogical. You cannot be in a pandemic that has not YET started, and you can only avert a crisis that has NOT YET taken place.
The current global coronavirus crisis is proof that global agencies such as the WHO can actually cause irreparable harm. Perhaps their global roles need to be called into serious question. “